|
Republic
of Latvia
Cabinet
Order No. 602
Adopted 23 October 2017
|
On the Plan in the Field of Rare Diseases 2017-2020
1. To approve the Plan in the Field of Rare Diseases for
2017-2020 (hereinafter - the Plan).
2. To determine that the responsible authority for the
management, co-ordination and supervision of the implementation
of the Plan is the Ministry of Health.
3. The authorities involved in the fulfilment of the Plan
shall prepare the information regarding the course of the
implementation of the Plan in 2018 and 2019, and submit it to the
Ministry of Health by 30 March of the following year
accordingly.
4. The Ministry of Health shall ensure the implementation of
the measures provided for in the Plan in 2017 and 2018 within the
framework of the allocated State budget resources. The issue of
allocating additional State budget resources to the Ministry of
Health for the implementation of the Plan in 2019-2020 shall be
examined by the Cabinet together with the requests for additional
financing submitted by all ministries and central State
institutions within the process of preparing and examining the
draft annual State budget and draft medium term budget framework
law.
5. The Ministry of Health shall draw up and the Minister for
Health shall, by 1 June 2021, submit to the Cabinet an
informative report on the fulfilment of the Plan in accordance
with the laid down procedures.
Prime Minister Māris Kučinskis
Minister for Health Anda Čakša
(Cabinet
Order No. 602
23 October 2017)
Plan in the Field of Rare Diseases 2017-2020
Riga 2017
Content
I. Summary
II. Background
2.1. Early and Timely Diagnostics of Rare Diseases
Problems to be Addressed
2.2. Timely Treatment and Health Care Co-ordination Oriented
to a Rare Disease Patient
Problems to be Addressed
2.3. Improvement of the Circulation of Information Regarding
Rare Diseases
Problems to be Addressed
III Targets and Tasks to be Performed
IV Assessment of the Impact on the State and Local Government
Budget
Abbreviations
| BKUS |
VSIA
"Bērnu klīniskā universitātes slimnīca" [State limited
liability company Childrenʼs Clinical University
Hospital] |
| BMC |
Latvian Biomedical
Research and Study Centre |
| CF |
Cystic
fibrosis |
| COMP |
Committee for
Orphan Medicinal Products |
| DNA |
Deoxyribonucleic
acid |
| EC |
European
Commission |
| EMA |
European Medicines
Agency |
| EU |
European
Union |
| ESF |
European Social
Fund |
| EHIC |
European Health
Insurance Card |
| IT |
Information
technologies |
| CUH |
Clinical
university hospitals |
| ALRP |
Association of
Latvian Rehabilitation Physicians |
| ALFP |
Association of
Latvian Family Physicians |
| ALRFP |
Association of
Latvian Rural Family Physicians |
| MoW |
Ministry of
Welfare |
| UL |
University of
Latvia |
| ARPOL |
Association of
Rehabilitation Professional Organisations of Latvia |
| Cabinet |
Cabinet |
| LR |
Law or
regulation |
| Regulation No.
1529 |
Cabinet Regulation
No. 1529 of 17 December 2013, Procedures for the Organisation
and Financing of Health Care |
| Regulation No.
746 |
Cabinet Regulation
No. 746 of 2 September 2008, Procedures for the
Establishment, Enlargement and Maintenance of the Register
for Patients Suffering from Certain Diseases |
| NHS |
National Health
Service |
| NGO |
Non-governmental
organisations |
| ORPHA code |
System for
codification of the RD |
| PAH |
Pulmonary arterial
hypertension |
| Plan |
Plan in the Field
of Rare Diseases 2017-2020 |
| PREDA |
System of the
register of patients suffering from certain diseases |
| PSKUS |
VSIA
"Paula Stradiņa klīniskā universitātes slimnīca"
[State limited liability company Pauls Stradins Clinical
University Hospital] |
| WHO |
World Health
Organisation |
| RAKUS |
Sabiedrība ar
ierobežotu atbildību "Rīgas Austrumu klīniskā
universitātes slimnīca" [limited liability company Riga
East Clinical University Hospital] |
| RD |
Rare diseases |
| RSU |
Rīga Stradiņš
University |
| S2 form |
S2 form
"Confirmation of the right to planned medical treatment" |
| CDPC |
Centre for Disease
Prevention and Control |
| ICD |
International
Statistical Classification of Diseases and Related Health
Problems |
| GDoLP |
Genome Database of
Latvian Population |
| MoH |
Ministry of
Health |
| CSPMP |
Compensation
system for the purchase of medicinal products |
I. Summary
The objective of the Public Health Policy Guidelines
2014-20201 (hereinafter - the Guidelines) is to
increase the number of healthy life years of inhabitants of
Latvia and to prevent premature death by preserving, improving
and restoring health. To achieve this, two of the sub-objectives
defined in the Guidelines provide for the following - to prevent
inequality in the field of health by taking measures to ensure
equal health care opportunities for inhabitants of Latvia, and
reduce premature mortality from non-communicable diseases by
reducing the negative impact of risk factors on health.
The Decision No 1295/1999/EC of the European Parliament and of
the Council of 29 April 1999 laid down the a Programme of
Community Action on Rare Diseases (hereinafter - the RD),
including genetic diseases. This programme defines that the RD
affects less than 5 per 10 000 persons in the EU. For the time
being, the number of RD established in the EU is five to eight
thousand, and 6 to 8 % of the inhabitants fall ill during their
life. Although the spread of each individual rare disease is low,
in total 27 to 36 million of the EU inhabitants suffer from them.
Most of them suffer from such rare diseases which affect one per
100 000 persons or even less. Thus these persons are especially
isolated and vulnerable. The RD should be viewed within the
context of the health and social care, because falling ill with
them changes the life quality of patients significantly by
causing severe and chronic health disorders in the most of the
cases. First symptoms of the illness may appear at any stage of
human life from the birth to old-age.
On 8 June 2009 the EU Council Recommendation (hereinafter -
the Council Recommendation) for the Members States on an action
in the field of the RD2, including the RD definition,
was approved. The Recommendation mainly focuses on the
definition, codification and accounting, research of rare
diseases, European reference networks, compilation of special
knowledge on the EU level, participation and sustainability of
patient organisations. According to the Recommendation each
Member State had to, as soon as possible, but preferably by the
end of 2013, elaborate and adopt a plan or strategy in the field
of RD that would become part of the health and social care
system.
In its turn, the Implementation report on the Commission
Communication on Rare Diseases of 2014 and Council Recommendation
of 8 June 2009 on an action in the field of rare
diseases3 provides an overview of the implementation
of the rare diseases strategy is presented, and looks at the
achievements and lessons learned. The report has been prepared to
establish the extent to which the measures referred to in the
Council Recommendation4 have been introduced and to
bring forward proposals for measures that should be implemented
in the future.
In order to implement the EU Council Recommendation on an
action in the field of the RD and make a uniform State policy,
and also to ensure work co-ordination, the Ministry of Health
approved the Plan in the Field of Rare Diseases 2013-2015 by
Order No. 110 (20 June 2013) which included the action plan with
laid down priorities and activities the implementation of which
was planned and performed within the framework of the present
budget.
The informative report On the Fulfilment of the Plan in the
Field of Rare Diseases 2013-20155 (hereinafter - the
report) concluded that although there is a possibility to carry
out genetic testing in Latvia, in the most cases they are not
within the range of the State paid services and patients may
carry out them outside Latvia by receiving S2 form in the cases
laid down in the laws and regulations, or for their private
funds. Taking into account the costs of examinations to be
carried out abroad and based on the cost-effectiveness
consideration it is necessary to create the procedures that would
give patients the possibility to carry out State paid
examinations in Latvia and use the S2 form only in specific
cases. Initially, it will require additional financial means, but
in medium-term it could be more cost-effective and ensure
availability of better genetic testing for patients.
In respect of drugs, within the period of previous Plan the
National Health Service analysed the reimbursement of medicinal
products for patients suffering from RD and concluded that the
information acquired from the databases at the disposal of the
institution does not permit clear identification of all the RD
(syndromes) in the ICD-10 and the orphan number due to different
use of the classification. Furthermore, the financing is not
provided within the framework of one specific programme. When
evaluating the possibilities for inclusion in the List of
Reimbursable Medicinal Products, the same clinical and economical
evaluation principles are applied to orphan medicinal products
(the limit for the incremental cost-effectiveness ratio - EUR 41
000 for additionally acquired year of life or year of life
without progression of the disease - equal for all medicinal
products), and also the evaluation of the effect on the budget of
the reimbursement system for the purchase of medicinal products
is the same as for other medicinal products. Thus the issue on
the access to drugs by the RD patients in conformity with their
diagnosis and severity level of the disease has not been solved
and is current for the time being.
In order to plan the budget funds in the long-term, the
information on the spread of the RD in the country and the number
of patients of the respective diagnosis is significant. The
report indicates that the amount of information included in the
Register of Patients who are Ill with Certain
Diseases6 in respect of the rare diseases does not
reflect the actual number of patients because the information is
not entered therein on regular basis. Therefore it is necessary
to seek for a solution which would ensure that the acquired
statistical data are credible and usable for the planning of
health budget.
By taking into account that laid down in the Council
Recommendation, and also to facilitate the achievement of the
sub-objectives laid down in the Guidelines, the Ministry of
Health has developed the short-term policy planning document Plan
in the Field of Rare Diseases 2017-2020 (hereinafter - the Plan)
which continues the activities commenced in the previous RD plan
for 2013-2015 by concurrently providing for additional funds for
the implementation of the activities included in the Plan.
The Plan has been developed in co-operation with the involved
public administration authorities - the CDPC, the NHS, NGO - the
Latvian Alliance for Rare Diseases, the Latvian Association of
the Specialists of Rare Diseases, the Latvian Association for
Human Medicinal Genetics and professionals of the sector (BKUS,
PSKUS, RAKUS, BMC).
Considering the present situation in the field of the RD, the
priority tasks and measures to be taken within the laid down time
period (2017-2020) are included in the Plan in order to improve
early and timely diagnostics of the RD, treatment thereof and
circulation of information on the RD, and they are intended to be
implemented in conformity with the laid down time schedule, and
also by taking into account both the necessary human resources,
work capacity, and allocated financing for the achievement of the
laid down objective.
II. Background
2.1. Early and Timely Diagnostics of
RD
The RD affect relatively small number of patients however they
seriously burden the health care system in the EU. Most of the RD
are genetic diseases, the rest of them are rare cancer diseases,
auto-immune diseases, congenital defects, toxic diseases and
infectious diseases. There is a lack of a specially adapted
health policy and special knowledge, therefore diagnostics is
late and health care is difficult to access. An erroneous or
non-existing diagnosis mostly denies the possibility to improve
life quality to thousands of RD patients.
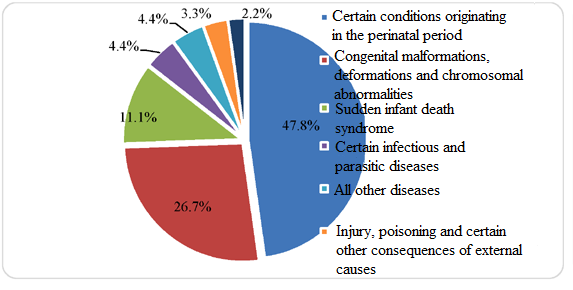
Congenital anomalies are the cause of death for more than the
fourth of the children who died during their first year of life.
Within the last years, no significant changes have been observed
in infant mortality due to congenital anomalies (1.1 per 1 000
live births in 2015 to 0.9 in 2014). However, by analysing the
indicator in a longer time period, it can be seen that it has
decreased from 2.3 per 1 000 live births in 2009 to 1.1 in
2015.
Main causes for infant mortality in Latvia in
20157
(share of all causes, %)
This could be partly explained by timely performance of
genetic tests, as a result of which it was possible to diagnose
congenital pathologies and to terminate a pregnancy by reducing
the risk of birth of seriously ill children, however in several
cases a pathology is diagnosed late, the pregnancy is aborted
after week 22, and these cases are included in the perinatal
mortality rates. Still, the number of congenital anomalies is
high which indicates that it is essential to improve the
diagnostics of perinatal congenital anomalies that would allow to
detect congenital pathologies more precisely, prepare for them or
end a pregnancy in cases of such pathologies where severe lasting
consequences are expected after prevention of the pathology.
Special attention also needs to be paid to the period before
conception, therefore the possibility to broaden genetic testing
that would allow to identify the possible risk factors in a
timely manner for both the parents-to-be and newborns should be
considered.
Most of the congenital malformations (birth defects) and
inborn errors of metabolism are separate pathologies and cannot
be diagnosed by carrying out only the external examination of
newborns, without using medicinal-genetic testing. Often a child
is discharged from the maternity ward too early, and the
diagnosis is established only after irreversible changes have
occurred in the organism and appropriate treatment cannot provide
the desirable result anymore. Timely diagnostics and commencement
of treatment have a determinative role in the issue of survival
or further development of a child. All abovementioned indicates
to the significant role of genetic prenatal and postnatal
diagnostics in the improvement of the population health and
reduction in the mortality rate. Latvia has an average of 20 000
newborns per year, and on average 40 children are born with
inborn errors of metabolism every year.
In respect of genetic testing the situation is similar.
Although genetic testing is available in the laboratory of the
BKUS, many of the tests provided in the Scientific Laboratory of
the Rīga Stradiņš University (hereinafter - the RSU) and the BMC
are not covered from the State budget resources. In conformity
with that laid down in the Plan in the Field of Rare Diseases
2013-2015 approved by Order of the Ministry of Health No. 110 (20
June 2013), representatives of genetic associations compiled
information on the DNA diagnostic methods that have approved
technologies and the commencement of the performance of which
would be desirable for the patients of the risk group, and which
could restrict the prevalence of congenital diseases in the
population by using invasive diagnostic methods in the early
stages of pregnancy, or to commence the necessary therapy in a
timely manner which, in turn, would provide for the possibility
to reduce the disability risk. Part of them was included as new
policy initiatives, however the State budget financing was not
allocated to them. For example, the Latvian Association of Human
Genetics has repeatedly addressed proposals to broaden the list
of the State paid tests with DNA diagnostic for several diseases
(see Table 1).
Table 1
|
Examination
|
Expected
number of examinations per year (cases)
|
Treatment
options
|
|
Haemophilia A DNA
diagnostics
|
10
|
Factor VIII
|
|
Haemophilia B DNA
diagnostics
|
5
|
Factor IX
|
| Based on the information
provided by the association, the incidence of Haemophilia A
is 1 per 5 000 boys which means that on average 2-3
Haemophilia A patients are born in Latvia every year. Whereas
the incidence of Haemophilia B is 1 per 25 000 boys which
means that on average 1-2 Haemophilia B patients are born in
Latvia every other year. |
|
dF508 and del394TT mutations
of cystic fibrosis CFTR gene
|
100
30
|
Antibacterial, mucolytic,
physiotherapy etc.
|
|
Full sequencing of the cystic
fibrosis CFTR gene
|
5
|
| The incidence of cystic
fibrosis is 1 per 3 300 children which means that on average
7 cystic fibrosis patients are born in Latvia every year.
Mutation del394TT must be determined only when dF508 is
negative in 30 % of the cases. |
|
C282Y and H63D mutations of
hereditary hemochromatosis HFE gene
|
20
|
Blood flush ensures complete
recovery of a patient (treatment with drugs is not
necessary).
|
| Patients do not require liver
biopsy for the diagnostics of the disease by carrying out the
venosection (by flushing the blood on regular basis, may be a
blood donor) - complete recovery is guaranteed. Therapy with
drugs or liver transplantation is not required. |
If the RD are caused by genetic changes, prenatal and
postnatal examinations that are paid from the State budget
resources can be carried out, for example, cytogenetic analysis
(chromosome analysis with a standard method and cytogenetic or
FISH method); biochemical genetic analysis: biochemical screening
of pregnant women of increased risk for genetic pathology of
foetus, mass neonatal screening for phenylketonuria and
congenital hypothyroidism, selective screening of inborn errors
of metabolism (analysis of amino acid spectrum, organic acid
spectrum, oligosaccharides, mucopolysaccharides and qualitative
carbohydrates); DNA diagnostics for spinal muscle atrophy,
hereditary motor sensory polyneuropathy, long-chain and medium
long-chain fatty acid oxidation defects, Huntington's chorea,
fragile X chromosome syndrome. Additionally, in Latvia the
diagnostics for CF hereditary hemochromatosis, Wilson's disease,
Gilbert's syndrome, alpha-1 antitrypsin deficiency, some types of
hereditary tumours, thrombophilias can be carried out within the
framework of scientific research projects or laboratories of
scientific institutions (at the moment polymorphisms of Gilbert's
syndrome and hemochromatosis are tested by private laboratories
in Latvia, but with a referral of the physician-specialist such
tests are covered from the State budget resources). It is not
always sufficient. For example, the Latvia Hemophilia Society
indicates that genotype analysis of the disease should be offered
to all patients with haemophilia of severe form and the results
obtained must be used in order to identify gene carrier in their
family.8
Despite the achievements in diagnostics of genetic diseases,
the number of patients with unspecified genetic pathology who
need additional testing abroad increases. Thus there is an
increasingly frequent co-operation with foreign laboratories and
clinics. Depending on the type of pathology, either the patients
themselves or only their biological material is sent for
consultations in foreign clinics and laboratories, and the
potential number of patients for whom the referral for the
specification of a diagnosis and treatment abroad would be
necessary is comparatively large and has the tendency to
increase.9
If any specific health care service is not available in Latvia
which, in turn, is available in other EU Member State, European
Economic Area state or Switzerland and this service is covered
from the State budget resources in Latvia, a person may request
S2 form "Confirmation of the right to planned treatment"
(hereinafter - the S2 form). The S2 form is a document of a
unified sample in all EU Member States. The S2 form is as a
guarantee that the country which has issued the S2 form to a
person will settle accounts with the EU Member State in which the
particular necessary planned health care service will be provided
for the person. The treatment will be provided under the same
care and payment conditions as are applied to the inhabitants of
the relevant country. This form is issued by the NHS.
Table 2
Number of issued S2 forms10
(during the time period 2006-2015)11
|
Year
|
Number of
issued S2 forms
|
|
2015
|
215
|
|
2014
|
231
|
|
2013
|
191
|
|
2012
|
173
|
|
2011
|
143
|
|
2010
|
104
|
|
2009
|
122
|
|
2008
|
127
|
|
2007
|
110
|
|
2006
|
26
|
205 administrative cases were examined in 2015. Of these, a
favourable decision has been taken in 196 administrative
cases12. In these 196 administrative cases, 70
decisions have been taken by recognising the right of the person
to receive health care services in Lithuania, 58 decisions - by
recognising the right of the person to receive health care
services in Germany and 41 decisions - to receive health care
services in Estonia. As in the previous years, the health care
service for the receipt of which in another Member State the
largest number of favourable decisions has been taken is genetic
analyses for children (50 favourable decisions have been taken in
2015). Based on the comparison of statistical data on the
increase of the number of administrative cases in long-term (in a
period of 5 years), it can be concluded that the number of
administrative cases has increased by 36.67 % (by comparing the
data of 2015 with the data of 2011).13 It cannot be
concluded from the abovementioned in how many cases of the RD the
S2 form is issued because this group of diseases is not
distinguished separately. It can be only indirectly considered by
examining the purpose for the issue of the S2 form.
Table 3
Planned health care services for the receipt of which in
another Member State a favourable administrative act has been
adopted and S2 form has been issued to a
person14
|
Type of
the health care service
|
Number of
services
|
| Genetic analyses (for
children) |
50
|
| Hymerism analysis for a person
after allogeneic stem cell transplantation |
26
|
| Eye surgery (brachytherapy of
beta applicators, transplantation of cornea etc.) |
22
|
| Search of stem cell donor,
allogeneic stem cell transplantation, in case of
complications - donor lymphocyte infusion and treatment of
complications |
22
|
| Monitoring and control of
minimum residual disease (MRD) after PCR (polymerase chain
reaction performed in actual time) in bone marrow aspirate
for the person with indications for allogeneic stem cell
transplantation |
14
|
| Physician consultation, where
necessary, diagnostics |
7
|
| Care after transplantation |
6
|
| Extracorporeal
photopheresis |
5
|
| Liver transplantation (for
children) |
4
|
| Laser ablation of blood vessel
anastomoses by performing the fetoscopy (for pregnant
women) |
3
|
| Separation of primary spinal
column tumour - neurofibroma - from spinal columns and
mediastinum Where necessary - stabilisation of spinal column
with implants from the front or back |
2
|
It follows from the abovementioned that the number of the S2
form recipients is rather limited because in the case of the RD
it is initially obvious that such examination method may not be
available in the country, because such cases are few and covering
from the State budget resources is to be evaluated additionally,
especially in case of a limited State budget financing as it is
in Latvia.
Upon evaluation of other possibilities for timely and early
diagnostics, the previous contribution and future potential of
the Genome Database of Latvian Population (hereinafter - the
GDoLP), the RSU and BKUS in the field of the RD must be noted.
Taking into account the significance of the RD diagnostics and
the necessity to work on the discovery of new methods, the genome
research has a significant role. The GDoLP creates and maintains
the BMC, and the purpose of it is to establish the base for
genetic material, and also other biologic material and
information base in order to improve detection and treatment of
different diseases (heart diseases, diabetes, cancer and many
other), and also in order to promote prevention of many diseases.
Until 2017, the GDoLP had accumulated samples of 31 504
inhabitants of Latvia , and it involves more than 2 000 new
patients every year, but the information and genetic material is
planned to be collected on 40 000-60 000 inhabitants of Latvia in
order to study how the human health is affected by their genes in
relation to the lifestyle and environment. The GDoLP is a
national level project which intends to establish a system for
surveying, maintaining and processing the health and genetic
information of the inhabitants of Latvia, and this system shall
serve for research, preventive and medical treatment
purposes.15
The GDoLP provides the possibility to inform the health care
organisers in Latvia of the number of ill persons or individuals
subject to a disease the cause of which is changes in genome.
Considering the abovementioned, at the national level the
planning of the diagnostic, therapeutic and preventive measures
for such diseases could be more efficient in the future. The DNA
examinations carried out within the GDoLP projects allow to
discover the mutations that are causing diseases not only after
emerging of the disease, but also before setting in of the
disease and also before the birth. As the DNA examination
technology (simultaneous analysis of many genes for a large
number of individuals and even finding out the individual genome
code) and the knowledge level of the public in genetics
increases, voluntarily DNA analysis of all individuals could
become possible. This would allow to detect in timely manner
those individuals who or offsprings of whom have a high risk of
the emergence of a genetic (monogenic or multifactorial) disease,
and also motivate to lead such lifestyle which would allow to
avoid the illness. Thus it would be possible to commence
treatment of the patient earlier, to prevent or limit
manifestation of the symptoms of the disease by retaining the
capacity for work of persons and saving the funds which would be
necessary for treatment and social benefits. In turn, by
establishing the relationship between persons genetic profile and
response to various drugs, the most appropriate drug for each
person can be selected, avoiding the side-effects thereof.
Since 2001, the Scientific Laboratory of Molecular Genetics of
the RSU has, within the framework of different scientific
projects, determined the most frequent genetic causes in the case
of Wilson's disease, cystic fibrosis, alpha-1 antitrypsin
deficiency and other monogenic pathologies. In the case of the
abovementioned pathologies, genetic analyses of family members
are also significant in order to carry out the DNA analysis while
still in the pre-symptomatic period when other examinations
cannot be carried out and, for example, in the case of Wilson's
disease, giving the possibility to commence treatment before a
liver damage has developed. As a result of the studies conducted
by the Scientific Laboratory of Molecular Genetics of the RSU the
most common genetic variations that are causing certain monogenic
pathologies in the population of Latvia have been established,
thus creating a DNA diagnostics algorithm that is suitable for
the population of Latvia in the case of Wilson's disease and
cystic fibrosis, and by continuing studies the DNA diagnostics
algorithms are also being developed in cases of other
diseases.
In its turn, BKUS as one of the first providers of diagnostics
of genetic diseases carries out molecular diagnostics of
Huntington's chorea, mutation analysis in GJB2 gene and K329E
mutation of medium-chain acyl-CoA dehydrogenase gene, molecular
diagnostics of fragile X chromosome syndrome, molecular
diagnostics of Charcot-Marie and hereditary compression
neuropathies, quantitative detection of MLL/AF4 chimeric gene
transcripts, quantitative detection of BCR/ABL chimeric gene
transcripts, detection of SNRPN gene methylation status, and also
detects SMA gene deletion, 1528G>C mutations of long-chain
3-hydroxyacyl-CoA dehydrogenase, mutations of phenylalanine
hydroxylase, dystrophin gene deletion, micro-deletion of Y
chromosome, MECP2 gene mutation, RYR1 gene mutation.
In relation to the RD health care the need to create data
"collections" of the RD patient biological material and related
clinical data, promoting the development of genetic tests and
research of these diseases and improvement of the treatment
thereof has been already confirmed. It provides the possibility
to perform investigation quickly and to find out genetic causes
of inheritance in the cases when the existing diagnostic tests
are unable to clarify it. It is especially important to
co-operate with similar bodies abroad to such aspect in order to
ensure the necessary number of samples for researches. The
availability of samples in biobank provides for the possibility
to additionally carry out genetic and biochemical examinations
for each patient if additional factors affecting the disease have
been detected.
Therefore the GDoLP with an already created system for the
processing of biological material and related data which includes
both the infrastructure and standardisation system of the
laboratory procedures is ready to create also the collection of
the RD samples. Accumulation and creation of such resources is
essential as due to rare incidence any biological sample obtained
and related information are especially valuable. By accumulating
material in a long-term a unified resource would be created for
the development of the RD diagnostics and treatment therapies in
the future. Concurrently, the participation of the GDoLP in the
Biobanking and BioMolecular Resources Research Infrastructure -
European Research Infrastructure Consortium (BBMRI-ERIC) which
enables exchange of the resources between biocollections of other
countries to the Consortium and would provide the possibility for
Latvia in the case of necessity for both to obtain the samples of
the RD patients and data from other countries and to participate
with them in research projects that would promote the RD research
and development of therapies in the world context.
Within the framework of research, one of the fields in which
the GDoLP is operating is acquisition of the molecular
diagnostics methods intended for the prognosis and selection of
therapy for hereditary diseases, research of demand and
cost-efficiency in Latvia. In co-operation with
physicians-specialists, the relevant pathologies are selected,
genome regions to be analysed or objectives of the examination
are identified, and the amount of patients to be analysed and
inclusion criteria are determined Based on the referrals by
physicians-specialists the relevant molecular examinations are
carried out, results of examinations are analysed by finding out
their efficiency and potential impact on therapy, and also by
accumulating the data on results and costs of the therapy in
long-term. Approbation of molecular diagnostic for several
pathologies has been carried out in the previous years, for
example comparative genome hybridisation for the detection of
large duplications or deletions of genetic material, development
of diagnostics panel for muscular dystrophies, full sequencing of
genes causing hypercholesterinemy, the method for determining
gene mutations which helps to evaluate the efficiency of
chemotherapy prognostically for the needs of onco-hematologists,
and also other examinations.
The problems to be addressed:
1) by taking into account that 80 % of the RD are congenital
and hereditary diseases which do not have specific preventive
measures, it would be necessary to find the possibility to ensure
genetic testing for the persons who are planning pregnancy, for
both parents-to-be in the anamnesis of whom there is any of
genetic diseases, or substantiated suspicions for the presence
thereof;
2) the availability of genetic testing shall be ensured not
only for children but also adult patients with relevant
indications that would allow to detect illness in a timely
manner, to commence treatment, that in turn would reduce the
disability risk (it refers also to the indications for granting
the S2 or E112 form for adult patients);
3) in order to improve the quality of RD diagnostics, it is
necessary to commence the DNA diagnostics for the most common
pathologies in Latvia by supplementing the list of the State paid
DNA diagnostic tests with the most common diseases of the North
European and East European populations for which the DNA
diagnostics has impact on the course of treatment, prognosis or
development;
4) based on the European experience, the research results and
resources of the GDoLP should be used more actively in the
prediction of diseases, planning of health care services and
diagnostics of diseases;
5) a registry of the RD patient biological material and
related clinical data should be created by involving the existing
infrastructures (within the framework of the GDoLP) for research
and genetic testing approbation purposes.
2.2. Timely Treatment and Health
Care Co-ordination Oriented to the RD Patient
The EU has adopted Regulation on orphan medicinal products
(Regulation (EC) No 141/2000 of the European Parliament and of
the Council of 16 December 1999 on orphan medicinal
products)16 the purpose of which is to facilitate to
develop orphan medicinal products. The centralised procedure for
the determination of orphan medicinal products is laid down
therein, and also incentives for the research, placing on the
market and improvement of orphan medicinal products (for example,
market exclusivity of 10 years, aid in accordance with protocol,
access to the centralised procedure for obtaining the marketing
authorisation) by which it is intended to facilitate research,
development and marketing of such medicinal products with which
rare diseases may be treated, prevented or diagnosed. Since
January 2014 the EC has recognised more than 90 orphan medicinal
products. It is important that the EC has recognised more than 1
000 products as orphan medicinal products17. Financers
who develop these products use these reliefs. They should such as
to relieve both the improvement of innovative medicinal products
and coming into the market of the medicinal products similar by
essence and recognition thereof for patients. During the last
years the number of denominations of medicinal products has
increased, in turn the number of authorisations has not changed
significantly (7 authorisations have been granted in 2013, in
turn in 2012 - 10). Concurrently it must be indicated that in
spite of different incentives the permitted orphan medicinal
products are not available in all EU Member States, and all
patients in all EU Member States do not have equal possibilities
to receive such medicinal products. Moreover their availability
is significantly delayed due to the lack of the financing.
Although decisions on the price and reimbursement are within the
competence of the countries, the Member States are facing
significant joint difficulties to ensure affordable, in terms of
costs, and sustainable access to medicinal
products.18
As indicated in the draft Council Conclusions19 on
strengthening the balance in the pharmaceutical systems in the EU
and its Member States, the legislation promoting the development
of orphan medicinal products, paediatric medicinal products and
advanced therapy medicinal products and granting marketing
authorisations, and also intending such reliefs for manufacturers
as supplementary protection certificates, data exclusivity or
market exclusivity, is in force for the time being. The draft
conclusions highlight that these reliefs need to be proportionate
to the goal of encouraging innovation development, improving
patients' access to innovative medicinal products with
therapeutic added value and budgetary impact. Creation of such
circumstances which might hinder the emergence of new or generic
medicinal products in the market and in this way limit patients'
access to new medicinal products should be avoided.
The EU Council indicates with concerns that after putting the
medicinal products on the market non-conformity with certain
requirements among the marketing authorisation holders is
observed which may cause the situation when the data of
independent researches and information from the patient registers
are not structured, compiled and made accessible to performers of
researches on efficiency and safety of medicinal products. And
also in several Member States the number of the cases when access
of a patient to efficient medicinal products is restricted by
high and non-permanent prices of medicinal products, taking out
medicinal products from turnover or non-putting new medicinal
products on the national market due to economic considerations.
Some Member States may be not sufficiently strong in individual
negotiations with pharmacy industry. Fragmentary granting of
marketing authorisations for new medicinal products, for example
for one medicinal product for small groups of patients or for one
active substance for the treatment of several rare diseases
promotes increase in prices of medicinal products. The
abovementioned problems should be referred not only to medicinal
products but also to medicinal devices. Besides, special
attention must be paid to the access to medicinal products by
patients in small Member States.
Data on the number of positive decisions taken by the COMP and
the number of medicinal products registered centrally with the
EMA indicate that during the first years of operation (2000-2010)
850 positive decision have been taken by the COMP, but the EMA
has registered 65 medicinal products for the treatment of the RD
during this period of time. 93 medicinal products for the
treatment of the RD have been registered by the centralised
registration procedures until 2016 of which 20 medicinal products
have been distributed in the market of medicinal products of
Latvia for EUR 2.5 million in total (the abovementioned medicinal
products have been covered within the framework of the CSPMP,
individual reimbursement and within the programme for the
treatment of rare diseases for children). The fact that almost
EUR 17 million have been used in total from the State budget in
2016, but EUR 2.5 million of them have been used for the payment
of the medicinal products especially intended for the treatment
of the RD, substantiates that parallels may not be drawn between
the division of the RD and patient needs and development and
approval of the medicinal products to which the status of the
medicinal products intended for the treatment of the RD is
granted.
In Latvia the compensation system for the purchase of
medicinal products (hereinafter - the CSPMP) ensures the
possibility for the patients to receive medicinal products and
medicinal devices that are necessary for the treatment of certain
diseases the purchase of which, fully or partly, is covered by
the State. Diseases for the treatment of which expenses for the
purchase of the medicinal products and medical devices are
reimbursed are laid down in the list of diagnosis of the diseases
which is the integral part of the compensation system for the
medicinal products. For the time being the medicinal products for
38 diagnoses of rare diseases are ensured within the framework of
the CSPMP. The medicinal products for the RD are included in the
list of reimbursable medicinal products which belong to the group
of the diseases of the blood and blood-forming organs and
disorders involving the immune mechanism, diseases of the skin
and subcutaneous, tumours, diseases of the respiratory system,
endocrine, nutritional and metabolic diseases, diseases of the
musculoskeletal system and connective tissue, congenital
diseases, mental and behavioural disorders. In 2016 the treatment
within the framework of the CSPMP was received by 5 100 unique
patients with rare diseases by using EUR 13.8 million from the
State budget. The largest financial means were used for the
treatment of haemophilia, juvenile arthritis, multiple sclerosis,
Turner syndrome and diseases related to changes in the production
of growth hormone (acromegaly, hypopituitarism). If diagnosis is
not included in the list or the necessary drug is not in the list
of reimbursable drugs for the treatment of a particular diseases,
patients may ask the State aid for the purchase of the medicinal
product in accordance with individual procedure. It shall be used
by patients with complications in the course of the disease, and
also by patients for whom rare diseases have been diagnosed. In
2016 the medicinal products have been reimbursed individually for
the following rare diagnoses or groups of diagnoses:
|
Diagnosis
|
Code of diagnosis
|
Unique patients
|
Financing, euro
|
| Disorders of copper
metabolism |
E83.0
|
39
|
11 025
|
| Systemic connective tissue
disorders |
M30-M35
|
5
|
26 516
|
| Multiple sclerosis |
G35
|
7
|
53 560
|
| Epilepsy, rare form |
G40
|
28
|
40 395
|
| Diseases of the blood and
blood-forming organs and disorders involving the immune
mechanism |
D35.2; D61; D69, D82-84
|
28
|
232 811
|
| Pulmonary hypertension |
I27
|
171
|
1 385 260
|
| Carcinoid tumour/carcinoid
syndrome |
C16-C80, D13
|
34
|
333 358
|
| Juvenile arthritis |
M08
|
1
|
5 178
|
| Congenital diseases |
Q05; Q24; Q44; Q55; Q78
|
16
|
7 814
|
|
Total
|
|
186
|
1 182 939
|
Patients must often use drugs the expenses of which exceed the
limits for individual reimbursement laid down by the State for
several times - in the amount of EUR 14 228.72 for one patient
during a period of 12 months. The abovementioned limit for
reimbursement precludes part of the patients from purchasing the
necessary drugs, it promotes inequality in the accessibility of
medicinal products and may lead to early mortality from rare
diseases among adult patients. Considering the abovementioned,
the Public Health Policy Guidelines 2014-2020 identified that in
order to reduce the cases of early death and disability of
inhabitants as a result of rare diseases and to ensure
accessibility of medicinal products to adult patients with rare
diseases by increasing the amount of the funds in the State
budget intended for the reimbursement of medicinal products, the
system for the compensation of medicinal products needs to be
reviewed:
1) by expanding the list of those diagnoses for which drugs
are compensated by the State with rare diseases diagnosed in
Latvia;
2) by expanding the list of reimbursable drugs with new drugs
including with drugs for the treatment of the RD;
3) by gradually increasing the amount if individual
reimbursement laid down in the State for the treatment of rare,
difficult and complicated diseases.20
Taking into account that medicinal products of the new
generation are expensive and costs thereof are not always
commensurate with the funding granted for the reimbursement of
medicinal products, the possibilities for inclusion of new
medicinal products in the system for the compensation of
medicinal products are limited. In order to promote improvement
of availability of new medicinal products, the development of the
CSPMP was intended in the Public Health Policy Guidelines
2014-2020, including enlargement of the system for reimbursement
of medicinal products with existing and new medicinal products by
indicating the financing necessary for it in 2015 in the amount
of EUR 4 280 000 and in 2016 in the amount of EUR 17 117 000, in
2017 in the amount of EUR 74 407 000. However, within the
framework of the law On the State Budget for 2015 the funds in
the amount of only EUR 2 536 431 have been granted for the
Ministry of Health for 2015 and following years for the
improvement of the system for reimbursable drugs and materials
and the system for the treatment of the RD with drugs for
children, including the funds in the amount of EUR 2 000 010 for
covering reimbursable medicinal products and materials which have
been directed for covering the deficit of funds lacking in the
compensation system of expenses for the purchase of medicinal
products not inclusion of new medicinal products in the
compensation system for the medicinal products. Unfortunately,
the development of the CSPMP laid down in the Public Health
Policy Guidelines 2014-2020 will be possible only if the
appropriate financing will be included in the law on the State
budget.
In respect of the availability of drugs for children the
sub-programme of the health care budget "Treatment of Rare
Diseases with Drugs for Children" ensures coverage of the costs
of the treatment with medicinal products for the children
suffering from the RD who are registered with the BKUS by
ensuring maintenance of important life functions. In 2015, EUR 1
990 076 were granted for this programme. 15 children with
diagnoses received treatment with drugs. Gaucher disease,
mucopolysaccharidosis type 1 and 2, urea cycle disorder disease,
Lesch-Nyhan syndrome, homocystinuria, inherited IX factor
deficit, phenylketonuria (classical form), Pompe disease,
tuberous sclerosis, other demyelinating diseases of central
nervous system, melanoma of scalp and neck21.
In turn, in order to improve availability of drugs to the RD
patients after 18 years of age by amending Cabinet Regulation No.
1529 of 10 January 2015, Procedures for the Organisation and
Financing of Health Care (hereinafter - Regulation No. 1529), the
stipulation "If the treatment with drugs has been commenced for a
child at the valsts sabiedrībā ar ierobežotu atbildību
"Bērnu klīniskā universitātes slimnīca" [State limited
liability company Childrenʼs Clinical University Hospital] from
the funds of the budget sub-programme "Treatment of Rare Diseases
with Drugs for Children" then it shall be continued after
reaching 18 years of age until such necessity terminates in
conformity with medical indications". However, it is necessary to
plan for an increase in the funds granted to this programme in
the long-term, because it should be taken into account that the
dose of drugs necessary for children is calculated per weight,
and it, in turn, means that by the growth of the child the costs
of drugs will increase. There is an opinion that these costs may
increase by 10 % per year on average. It must be taken into
account that by improvement of diagnostics children with other
diagnoses of rare diseases may be included in this programme (2-3
new patients per year on average) that could increase the total
costs by 25-30 %.
In addition to the abovementioned, this programme should
provide resources also for special therapeutic nutrition which is
one of the determining factors during the treatment process in
the case of the RD diseases and ensures the stability of
metabolic condition of the patient and consecutive growth and
psychomotor development of the child by minimising the risk of
disability. Already now the laws and regulations22
determine the provisions for therapeutic nutrition for the
patients with cow milk protein intolerance of severe degree and
malabsorption syndrome of severe degree, palliative care patients
and CF patients, but there is a range of metabolism, genetic and
neurological disorders which need special enteral nutrition which
is the part of both the therapy and also significant condition
for maintaining the life. For example, for the treatment of
refractory forms of epilepsy the so-called ketogenic diet with
high content of fatty substances and low content of
carbohydrates, and also normal amount of calories must be
followed. In accordance with the data of the Association of
Pediatric Neurologists, there could be five such patients per
year. Costs per one patient would amount to EUR 500 per
month.
The Public Health Policy Guidelines 2014-2020 lay down that
the receipt of lung transplantation service should be ensured. At
the moment, lung transplantation surgery is not a health care
service that is paid from the State budget in Latvia, although
there are patients who are suffering from diseases for which lung
transplantation is required, for example, pulmonal arterial
hypertension (hereinafter - the PAH) patients. The PAH can
develop at any age, also with children, however most often it
emerges among young women. In turn, mortality in the case of the
PAH is as high as with different cancer forms, including breast
and colorectal cancer. The most important examination (screening
examination) in diagnostics of pulmonary hypertension is
echocardiography which in the case of necessity is followed by
heart sensing, after which, if necessary, the pathogenetic
disease therapy is designated for the patient.
Complications in bronchopulmonary system irreversibly develop
for the CF patients (at the moment, 42 patients). Most of them
will need lung transplantation. Lung transplantation is carried
out for young patients with a lung disease in a late stage
(progressive obstructive, fibrotic or pulmonary vascular disease
with high risk of mortality within the next 2-3 years) for whom
classical and alternative treatment methods are inefficient, thus
preventing deterioration of the health condition, capacity for
work and setting in of disability for the patients, and improving
their quality and duration of life. The Ministry of Health has
repeatedly requested this measure and the additional State budget
financing necessary for its implementation in the list of new
policy initiatives for 2016-2018, and its implementation is
dependent on the financial possibilities of the State budget.
To ensure qualitative care, a multi-disciplinary approach is
significant in the care of the RD patients that would ensure the
most suitable aid for each particular patient. Within its
framework, an individual treatment, care and rehabilitation plan
could be made for each patient, including the necessity for the
receipt of new medicinal products and medicinal products for the
treatment of rarely occurring diseases (orphan medicinal
products) would be evaluated. In order to provide suitable aid to
the RD patients, a specialist must invest more work to go deeper
into the particular problem, and also to understand and recognise
it as an exception by concurrently continuing to search for
answers to unclear questions by sharing experience with other
specialists. Such approach may extend the duration of a visit,
and thus increase the fee for the service.
For the time being unified principles for the establishment of
multi-disciplinary team cannot be developed as in each case of
illness different health care specialists may need to be
attracted. For example, in accordance with the agreement entered
into on the provision of the State paid health care services,
certain amount of financing is granted to the Palliative Care and
CF room at the BKUS within the framework of which the medical
treatment institution may attract the necessary specialists. In
2015, the health care services in the palliative care room were
provided by a child care nurse, oncology care nurse,
pediatrician, nurse, pediatric hematologist-oncologist,
psychologist, neurologist, surgeon, oncologist-chemotherapist,
assistant to physician and family (general practice) physician.
Whereas, in 2015, the health care services in the CF room were
provided by a pediatric gastro-enterologist, pediatric
pneumonologist, pediatrician, child care nurse, dietologist,
family (general practice) physician. However, the general
procedures laid down in Regulation No 1529 also provide that a
patient may be sent to other specialist in the case of
necessity.
In conformity with that laid down in the Council
Recommendation in the field of the RD, the Member States should,
by the end of 2013, survey suitable national special knowledge
centres in the territory of their country and promote
establishment of special knowledge centres which would organise
care of such patients who are suffering from rare diseases by
ensuring the co-operation with the relevant experts and
performing exchange of professionals and knowledge on the
national level or in the case of necessity with other
countries23.
It must be noted that access of the Member States to
organising expert-examination centres in their health care
systems has been very diverse. Some countries have officially
selected expert-examination centres in the field of the RD
(France, Denmark, Spain and United Kingdom). Regional
expert-examination centres in the field of the RD have been
established in Italy. Selection criteria in each country are
different and sometimes they are not equal even within the
framework of the regions of one country, although these criteria
often comply with Quality Criteria for Centres of Expertise for
Rare Diseases in Member States of 24 October 2011 developed in
the field of rare diseases by the EU expert
committee.24
Until now, involvement of medical treatment institution in the
establishment of national level centres in the field of the RD
has been based on the voluntary principle and additional
financing has not been provided, thus in Latvia medical treatment
institutions have not taken significant activities. The CF room
which is functioning in BKUS since January 2014 must be mentioned
as a positive example. A multi-disciplinary team (pediatric
pulmonoligists, nutrition specialist, physiotherapist,
psychologist, gastro-enterologist, the CF nurse) has been
established for the care of the CF patients. Further education of
medical staff takes place on regular basis, a pediatric
pulmonologist - CF specialist has been trained. Within the
framework of the State paid programme, treatment of both the
children and adults is provided free of charge to the CF
patients, and the range of administered drugs is being broadened
as much as possible. Inhalers and therapeutic nutrition is
available to the CF patients free of charge. During the last
three years the BKUS has organised educational lectures on CF for
the CF patients and their family members, and informative
materials have been created and are available for the patients.
The doctors' councils are organised for in-patients once a
month.
In addition to the abovementioned, upon an increase in
awareness of both patients and specialists, the BKUS has surveyed
its possibilities on how to ensure appropriate flow of the RD
patients and continuity of the health care, and has supported
establishment of the RD centre (hereinafter - the Centre) as a
co-ordination centre on the BKUS base by establishing support
"units" in other clinical university hospitals (hereinafter - the
CUH).
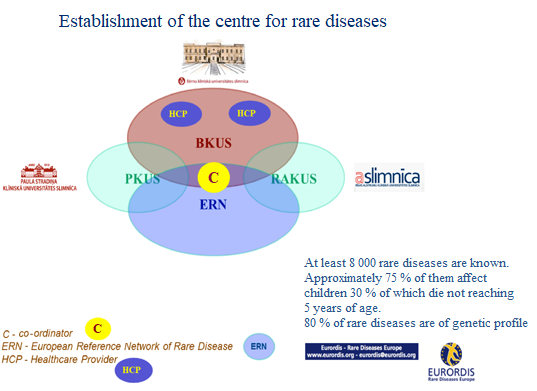
Establishment of such Centre would ensure centralised
availability of information and treatment for patients, focused
and efficient use of the existing resources for the RD
diagnostics and possible treatment of patients, the co-operation
with ERN (European Reference Network) for the treatment of
the patients and improving qualification of the professionals of
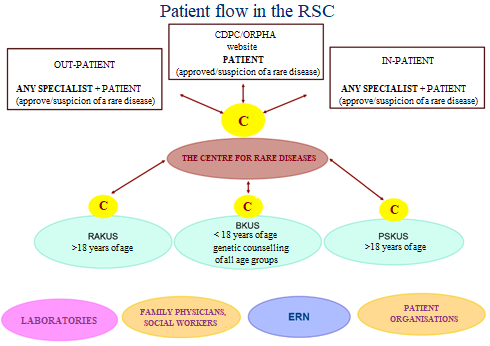
Latvia.25 At least one co-ordinator could operate in
the Centre and other CUH for organising patient flows and
attraction of specialists. In addition to the abovementioned all
CUH must agree on the rare diseases or groups of diseases the
treatment of which they can provide. Thus the competences between
involved hospitals would be determined and the work of
co-ordinators would be initially simplified by assessing the
possibilities for the referral of the patient.
To ensure efficient and up-to-date patient care, one of the
current problems is the improvement of medical treatment
competences and skills in RD. Without experience and appropriate
training it is not possible to detect diagnosis in a timely
manner and commence the necessary therapy. In certain cases it
may be decisive, causing irreversible changes in the health
condition of the patient by accelerating the possibility for
causing a disability. The CUH shall organise post-graduate
training courses, seminars and conferences on regular basis for
different health care specialists which contain also the RD. For
example, within the framework of the Third Baltic Pediatric
Congress (19-21 September 2015) in Riga, a separate section was
devoted to the RD in which issues of mucopolysaccharidosis,
Gaucher disease and Fabry disease, rare iron-deficiency anaemia,
homocystinuria etc., including a presentation on the experience
of Latvia in the health care of the CF patients has been
provided.
Significant educational work in the field of the RD has been
carried out also by the Latvian Association of the Specialists of
Rare Diseases. On 1 October 2016 the First Rare Disease
Conference of Latvia took place in co-operation with the
Department of Internal Diseases of the RSU and Rare Disease
Research Foundation within the framework of which general
knowledge on rare diseases and possibilities for diagnostics and
treatment thereof in Latvia, and also the information on the rare
diseases diagnosed and treated for patients in Latvia - pulmonary
hypertension, Fabry disease, Wilson's disease, Idiopathic
pulmonary fibrosis, Primary amyloidosis and Porphyria, was
provided. In turn, on 22 April 2017 the Second Rare Disease
Conference of Latvia was organised with a goal to provide
theoretical and practical knowledge on rare diseases, diagnostics
and treatment possibilities thereof for both the present
specialists and future specialists.
In addition to that, medical practitioners have a possibility
to take part in annual "summer schools" which are organised by
the specialists of the RD centre of Italy. In this training
particular RDs are not discussed, but the participants are
informed of the joint European approach to addressing RD issues -
their accounting, coding, development of guidelines, and also
organisation of the health care availability for such patients,
including ensuring the continuity of the health care for young
people when they are transferring to adult health care.
Problems to be Addressed:
1) in co-operation with specialists it is necessary to
determine the RD or groups of diseases for which therapy is
available and adequate treatment needs to be provided in order to
carry out assessment of possible reimbursement for medicinal
products and/or therapeutic nutrition;
2) in order to retain the present approach and CDPMP for more
occurring diseases, it would be purposeful to establish a
separate programme for treatment with drugs for adult patients
with a separate independent financing as it is in the case of
programme "Treatment of Rare Diseases with Drugs for Children" of
the BKUS;
3) it is necessary to introduce regular evaluation of clinical
efficiency of the drugs prescribed to RD patients based on
predetermined criteria which would provide the possibility for
the doctors' council to decide on continuing the commenced
therapy or necessity to change it;
4) clear and explicit criteria must be developed for the
inclusion of children with RD in the programme "Treatment of Rare
Diseases with Drugs for Children" and exclusion therefrom, and
also additional financial means must be provided for in the State
budget for the optimal functioning of this programme;
5) clear and explicit criteria must be developed for the
inclusion of adults with RD in the programme for the treatment of
the RD and exclusion therefrom,
6) coverage of the therapeutic nutrition should be provided
from the State budget resources to all those RD patients for whom
it is the only means of nutrition and which may not be replaced
by another nutrition;
7) by taking into account that mutual co-operation of
specialists (family physicians, gynaecologists, paediatricians,
endocrinologists, internists, cardiologists, pulmonologists and
other specialists) and their knowledge are essential for the
recognition of the RD recommendations for both the prophylactic
measures and recognition, diagnostics and treatment of the RD
need to be developed;
8) knowledge of medicinal practitioners regarding the
recognition of the RD must be broaden and strengthened by
organising clinical conferences with case studies and exchange of
experience, seminars, further education courses by involving the
specialists of different profile, including geneticians;
9) the flow of the RD patients must be improved especially by
ensuring the transfer of patients to adult health care by
strengthening the work of the RD Centre and special "units" in
CUH.
2.3. Improvement of the Circulation
of Information regarding the RD
Council Recommendation on an action in the field of rare
diseases26 lays down that it should be tried to ensure
that the RD are appropriately codified and can be found in all
health protection information systems, thus promoting that the
disease is duly recognised in the health care systems and
compensation systems for the purchase of medicinal products on
the basis of the International Classification of Diseases and in
compliance with the national procedures.27
At the moment, all the Member States use the International
Classification of Disease ICD-9 or ICD-10 systems in which the
most part of the RD is not mentioned. Some Member States
(including Latvia) have introduced ORPHA codes (RD codification
system which is developed by the Orphanet network28)
in their systems of the health statistics concurrently with the
IDC nomenclature or as a pilot project. In order to compile and
publish information on the RD, the Commission supported Orphanet
Joint Action29 through the EU Health Programme by
involving all the Member States as associated or co-operation
partners. Orphanet is a database that is available in seven
languages and has been established with a view to link
information on more than 6000 diseases. Besides each country has
its own section in the language of the relevant country in the
Orphanet portal.30
Additionally it must be taken into account the Joint Research
Centre of the EC, in order to ensure mutual use, comparison and
combability of the present 588 RD registers (62 European, 35
worldwide, 423 national, 65 regional and 3 non-specified
registers), is developing the European platform for the
registration of the RD, the most important tasks of which is to
ensure the main point of access where all interested parties
could receive information on the registers of the RD patients, to
support new and existing registers by taking into account their
mutual use, and to ensure IT tools for the maintenance of the
data compilation and operations of supervisory
networks.31. In the future it could ensure entry of
all data online, and also the information not only on each Member
State, but also on the EU in general in the field of the RD.
Taking into account that at the moment in Latvia the RD
patients are not accounted in a comprehensive and correct manner,
it is impossible to effectively compile information on the RD.
Such information would allow to plan the necessary State aid for
the diagnostics of the RD patients, their treatment, care and
rehabilitation. The lack of accounting not only hinders the
commencement and direction of purposeful and planned actions, but
also prevents the identification and addressing of the existing
problems by not allowing to make an objective assessment of their
scope and the level of severity.32
Procedures for supplementing and keeping the registers of
patients who are ill with certain diseases are determined by
Cabinet Regulation No. 746 of 15 September 2008, Procedures for
Developing, Supplementing and Maintaining Register of Patients
who are Ill with Certain Diseases (hereinafter - Regulation No.
746). The manager and holder of the registers is the Centre for
Disease Prevention and Control (hereinafter - the CDPC) which
ensures operation of the registers and enters into agreements
with medical treatment institutions on personal data processing
and protection.
Unfortunately, the information included in the register at the
moment does not reflect the actual number of patients, as the
information is not entered on regular basis. Although the
procedures for the provision of the information on the cases of
certain diseases to the CDPC in order for the necessary data to
be included in the registers are laid down in laws and
regulations, the accounting of the RD is being carried out based
on the internal resources of each medical treatment institution.
Data entry is also affected by the fact that the patients of the
CUH receive health care services from different specialist at
different medical treatment institutions, thus one person who
would be responsible for the data entry has not been determined.
Moreover, physicians are not motivated to fill out registration
cards of the patients who are ill with certain diseases due to
large workload.
In discussions with specialists of this field and
representatives of the CDPC, the possibility to gradually
establish the RD register on the base of the Register of
Congenital Diseases. By Cabinet Regulation No. 206 of 22 April
2014, Amendments to Cabinet Regulation No. 746 of 15 September
2008, Procedures for Developing, Supplementing and Maintaining
Register of Patients who are Ill with Certain Diseases, the
amendments to the Register of Patients who are Ill with Certain
Diseases have been approved by providing that the oncological
patient's registration card and registration card for a patient
with congenital anomalies is being supplemented with the
information on the RD code and name in conformity with the RD
classification on Orphanet. Thus medical practitioners of CUH,
being under contractual relations with the CDPC, have the
possibility to enter the information on diagnosed RD online.
Already now, in registering new cases of congenital anomalies,
the possibility to apply orhpa code is evaluated - if the
detected diagnose complies with the RD, the specialist
(genetician) assigns the appropriate orpha code. 1240 unique
entries have been registered in total until 14 June 2017 for
which any of the RD has been indicated (see Table No. 4).
Table 4
Number of cases registered in
the Register of Congenital Anomalies from 2011 to
201733
|
Year of
birth
|
Number of
unique entries
|
Number of
diagnoses
|
including
|
|
Number of
diagnoses with RD code (Orpha code)
|
Number of
unique entries with RD code (Orpha code)
|
|
In total until 2010
|
-
|
-
|
653
|
639
|
|
2011
|
537
|
745
|
56
|
56
|
|
2012
|
509
|
744
|
70
|
68
|
|
2013
|
515
|
829
|
80
|
80
|
|
2014
|
529
|
881
|
108
|
108
|
|
2015
|
436
|
590
|
109
|
106
|
|
2016
|
308
|
514
|
141
|
139
|
|
2017
|
72
|
109
|
46
|
44
|
In conformity with the data of the Register of Congenital
Anomalies (where the RD are also registered) 324 rare diseases in
total have been registered as of 14.06.2017 (Orpha codes) for 1
108 patients of which 241 are adults (year of the birth up to
1998) and 867 children (year of the birth 1999-2017). Of which
the most often Orpha diagnoses for children (where 15 and more
cases have been registered) are phenylketonuria (40), haemophilia
A (32), polydactyly (52), CF (29), Duchenne-Becker Muscular
Dystrophy (24), congenital hydronephrosis (27), congenital ptosis
(27), congenital cataract of different localisation (60),
juvenile rheumatoid arthritis (16), hypospadia (16). In turn, in
respect of adults (for whom 15 and more cases have been
registered) - phenylketonuria (42), haemophilia A (27), Wilson's
(3) and Fabry (17) diseases.
By developing and gradually introducing the Electronic
Information System of the Health Care the existing information
systems are included in the unified platform - the system for the
registration of patients who are ill with certain diseases PREDA,
NHS management information system which would allow to connect
the information included in different databases and to track the
RD patient according to both the received health care services
and prescribed drugs and efficiency thereof. In turn, by gradual
increasing the level of the knowledge of physicians-specialists
and linking the ICD-10 code to orpha code the number of the RD
patients and prevalence of diseases could be tracked
systematically.
In addition to the abovementioned, RD-Connect which is the EU
financed integration platform for joining the databases,
registers, biobanks and clinical bioinformatics in the field of
rare diseases34 organises practical seminars for civil
servants, specialists and patient organisations in order to
promote modern use of IT-solutions in the health data processing.
In 2016, the Latvia Hemophilia Society which now develops a
separate patient register for persons with congenital blood
coagulation disorders participated in such seminar at its own
expense.
In order to promote dissemination of knowledge and
information, the website devoted to the RD - Orphanet, ,
the multilingual portal, has been established within the
framework of the EC projects where the information on more than
5000 RD and medicinal products for the treatment thereof, newest
epidemiological data, studies on the spread of the RD in Europe
is available free of charge. The following services are available
on the portal:
- RD and RD classification which is developed based on the
published expert classifications;
- RD encyclopaedia (for patients, professionals) in English
and French which gradually is being translated in other languages
of the Member States;
- the list of orphan medicinal products in all stages of the
development thereof starting from granting of the status of the
EMA orphan medicinal product until obtaining the licence for the
European market;
- the list of specialised services which include information
on expert-examination centres, medicinal laboratories, research
projects, clinical researches, registers, co-operation networks,
technology platforms and patient organisations which operate in
the field of the RD in each Member State of Orphanet ;
- support instrument for the determination of a diagnosis
which ensures search according to symptoms and features of the
disease;
- encyclopedia of recommendations and guidelines for emergency
medical assistance and anesthesia;
- news issue OrphaNews (published once in two months)
which provides a summary on current events in the field of the
research and policy of the RD and orphan medicinal products in
English and French language;
- a collection of topical reports The Orphanet Reports
Serieswhere multidisciplinary themes are discussed and which
can be downloaded directly from the website35.

In conformity with the delegation of the Ministry of Health
the CDPC ensured the co-ordination of the Joint Action project No
2010 22 06 "Establishment of the European Network for Rare
Diseases and Orphan Medicinal Products" and management thereof in
Latvia. The Latvian part of Orphanet portal has been established
within the framework of the project where the CDPC in
co-operation with the Ministry of Health, patient organisations
and other bodies updates and publishes information in Latvian on
regular basis regarding the measures and current events in the
field of the RD. A new section has been established in the portal
with useful information for patients, their relatives and medical
practitioners. Three informative booklets are available on this
Section (diagnostics and care of spinal muscle atrophy (SMA)
patients; information for families on medical care for congenital
muscular dystrophy (CMD); recommendations for parents on
diagnostics and care of Duchenne muscular dystrophy (DMD)),
animation of the RD - porphyria symptoms, and also the
recommendations for primary prophylaxis of congenital anomalies
have been published.
In order to continue the commenced activities, the CDPC has
involved itself as the associated partner in the implementation
of the grant No. 677024 of the project of a third Programme of
the EC for the Union's action in the field of health (2014-2020
"Promoting Implementation of Recommendations on Policy,
Information and Data for Rare Diseases" (hereinafter - the
Project RD-ACTION). Period for the implementation of the project
is 1 June 2015 - 31 May 2018. The CDPC operates in the
implementation of the 4th work package. A participation in the
joint action project will ensure participation in the
international network Orphanet on the RD and orphan medicinal
products that would allow to use the infrastructure and resources
of the network Orphanet by ensuring the public of Latvia
(patients and specialists) with information on the RD because the
section of current events in the field of the RD will be
maintained and supplemented in the Latvian language on the portal
Orphanet. Being aware that within the framework of the network
Orphanet exchange of information is ensured on the international
level, the information on the expert-examination centres
recognised in Latvia in the field of the RD, specialists thereof,
patient organisations and laboratories which carry out specific
examinations will be updated on the databases of the Orphanet
within the framework of the project.
In considering the free flow of patients, the issue on
recognisability of the RD patients is topical, especially, if the
patient lives outside Riga and travels within Latvia and outside
Latvia, and if special knowledge is necessary for the treatment
of the particular RD or even urgent action is required when the
disease aggravates or there are complications. For ten years now,
upon such request, the Latvia Hemophilia Society provides
patients and medical institutions with Hemophilia Patient ID
cards, which include information about patients, their diagnosis,
severity of disease, drugs used for the treatment, as well as
contact details of medical treatment institutions for cases when
urgent action is necessary, but there is lack of required skills
and knowledge. Information is presented in both Latvian and
English which facilitates the travelling possibilities of a
patient.
Certainly such card could simplify receipt of a health care
service by the RD patient, especially, if the patient is outside
his or her place of residence or is travelling, and if the RD
from which he or she suffers is characterised by specific aid of
drugs in case the disease aggravates or other emergencies occur.
Its introduction could be commenced gradually and, possibly, also
voluntarily, by taking into account that the RD patient card
would contain sensitive patient data.
The experience of health care specialists of Portugal must be
mentioned as a positive example in the introduction of the RD
patient card. Before such card is issued a patient's consent is
received for access to his or her medical data. In the example of
Portugal, the information on the patient, attending physician and
orpha code of the disease are provided on the card. In turn, the
recommendation in the case of aggravation of the disease , and
also a contact telephone number which may be used in the cases of
uncertainties or emergency are indicated on the other side of the
card.36
Problems to be Addressed:
1) the accounting (registration) of the RD laid down in laws
and regulations must be ensured;
2) to increase knowledge of both the public and medical
practitioners on Orphanet database and the possibilities for
using the information included therein;
3) to increase and strengthen knowledge on the recognition of
rare diseases among medical practitioners regardless of their
speciality and medical treatment institution where a specialist
works (including at the places of imprisonment);
4) irrespective of advantages of e-health in the traceability
of patients, the possibility to issue approved patient cards in
common form, either by centralised procedure or authorising
patient organisations, must be evaluated for those patients of
rare diseases who have expressed the will to obtain such.
IV. Assessment of the Impact on the State and Local
Government Budget
(allocation of the financing is
provided in annex)
In order to implement the measures referred to in the Plan and
improve early and timely diagnostics and treatment of the RD and
the circulation of information on the RD, additional State budget
financing in the amount of EUR 66 866 490 is necessary for the
implementation of the Plan; the following amounts of this sum are
required each year: in 2018 - EUR 5 028 474, in 2019 - EUR 31 357
099, in 2020 - EUR 30 480 917, and every subsequent year
additional financing in the amount of EUR 30 499 917 is
necessary.
For early and timely diagnostics the additional financing of
EUR 1 846 549 (for 2018-2020) is necessary in order to improve
the availability of the RD diagnostics and broaden the range of
examinations covered from the State budget funds (for prenatal
and postnatal diagnostics, biochemical screening methods of
metabolic diseases).
The additional financing in the amount of EUR 64 798 036 (for
2018-2020) is necessary for the RD patient oriented timely
treatment and health care co-ordination. EUR 7 631 589 of this
sum are intended for the establishment of a special programme for
the treatment of adult RD with drugs that would have separate
financing which would allow to response more flexibly to the
needs of the RD patients by including new medicinal products
therein and to track the results of therapy and analyse them, the
improvement of the operation of the programme "Treatment of Rare
Diseases with Drugs for Children" EUR 55 245 389, for ensuring
research of medicinal products for the RD patients by transfer
from paediatric care (18 years) to adult care EUR 180 000. In
turn, EUR 1 024 000 are necessary in order to include lung
transplantation and pulmonary endarterectomy in the health care
services covered by the State by reviewing the tariffs of care
episodes and manipulations included in the health care service
and the procedures for the coverage of reimbursable medicinal
products. In order to determine the specialists included in the
multi-disciplinary team and the amount of health care service
provided by the, and also the procedures for the payment thereof
EUR 116 702 EUR 532 836 of the total financing for the activity
are necessary in order to strengthen the co-ordination of the RD
patient flow by establishing the RD centre with the BKUS and
co-ordination support "units" with the PKUS and RAKUS and EUR 67
520 for the provision of the methodological management of the RD
by developing the recommendations for the RD diagnostics,
treatment and dynamic observation (clinical algorithms and RD
patient "roadmaps").
Additional EUR 221 905 (for 2018-2020) are planned for the
improvement of information circulation on the RD in order to
create the RD patient card and linking thereof with EHIC to be
issued for the time being.
The Plan provides also the measures which will be implemented
within the framework of the State budget resources allocated to
the involved authorities for the implementation of the measures
(tasks) within the competence thereof.
1 Public Health Policy Guidelines 2014-2020;
2 Council Recommendation of 8 June 2009 on an
action in the field of rare diseases (2009/C 151/02)
3 COM(2014) 548
4 Council Recommendation of 8 June 2009 on an
action in the field of rare diseases (2009/C 151/02)
5
http://www.vm.gov.lv/lv/tava_veseliba/retas_slimibas1/
6
https://likumi.lv/ta/en/en/id/181288-procedures-for-developing-supplementing-and-maintaining-register-of-patients-who-are-ill-with-certain-diseases
7 Database of causes of death of the inhabitants
of Latvia
8
http://static.ehc.eu/wp-content/uploads/12-Recommendations-Wild-Bad-Kreuth-IV-initiative.pdf
9 Plan in the Field of Rare Diseases 2013-2015
10 The number of issued S2 forms does not match
with the number of the examined administrative cases due to the
fact that two or more S2 forms may be issued within the framework
of one administrative case (for example, the right to receive
several different health care services may be granted within the
framework of one administrative case).
11
http://www.vmnvd.gov.lv/lv/publikacijas/vestis
12 During the time period from 23 October 2013 to
31 December 2013 - 1 submission was received, during the time
period from 1 January 2014 to 31 December 2014 - 9 submissions
were received, during the time period from 1 January 2015 to 31
December 2016 - 28 submissions were received.
13
http://www.vmnvd.gov.lv/lv/publikacijas/vestis
14
http://www.vmnvd.gov.lv/lv/publikacijas/vestis
15
http://bmc.biomed.lu.lv/gene/KASirgenomadatubaze.htm
16 http://eur-lex.europa.eu
17
http://ec.europa.eu/health/human-use/orphan-medicines/index_en.htm
18 COM(2014) 548
19 Council of the EU. Council Conclusions on
strengthening the balance in the pharmaceutical systems in the EU
and its Member States, June 2016-
http://www.consilium.europa.eu/en/press/press-releases/2016/06/17-epsco-conclusions-balance-pharmaceutical-system
20 Public Health Policy Guidelines 2014-2020;
21
http://www.vmnvd.gov.lv/lv/publikacijas/vestis
22 Cabinet Regulation No. 1529 of 17 December
2013, Procedures for the Organisation and Financing of Health
Care
23 Council Recommendation of 8 June 2009 on an
action in the field of rare diseases (2009/C 151/02)
24 http://www.eucerd.eu/?page_id=13
25 The information provided by the BKUS
26 Council Recommendation of 8 June 2009 on an
action in the field of rare diseases (2009/C 151/02)
27 2009/C 151/02
28 http://www.orpha.net
29
http://ec.europa.eu/eahc/projects/database.html?prjno=20102206
30 COM(2014) 548
31 COM(2014) 548
32 Plan in the Field of Rare Diseases
2013-2015
33 Information from the Register of Congenital
Anomalies held by the CDPC (the information of live births and
medicinal abortions has been included, data as of 16.06.2017).
When necessary, the information regarding the newly discovered
cases is updated, and also entry of the data for 2016-2017 is
being continued.
34 http://rd-connect.eu/
35
http://www.orpha.net/national/LV-LV/index/par-orphanet/
36
http://www.sciencedirect.com/science/article/pii/S1877050915027283
Minister for Health Anda Čakša
Translation © 2018 Valsts valodas centrs (State
Language Centre)








